
Supplements for Women in Their 30s: A Short, Tested List
You've probably typed something like "best supplements for women in their 30s" into a search bar, then closed the tab. The results all push fifteen bottles, every one of them "essential." That's not a routine. That's a shopping list someone else profits from.
Here's our take, the shorter and honest version. For most women in their 30s, a small handful of supplements earn their place, and the rest are noise. The two that matter most are iron and folate. Low iron is one of the most missed shortfalls in women who still get a period. It drains your energy long before a standard blood test calls you "anemic." Folate is the other. Started before you're pregnant, it can prevent most neural tube defects.2 These are serious birth defects that form in the first few weeks after conception, often before you know you've conceived.
Everything else on this page comes down to one rule. Test before you supplement, and correct only what's low. That single habit will save you more money, and do more for how you feel, than any "women's multivitamin" on the shelf.
What changes in your 30s
Your 30s aren't a cliff. Most of the big shifts are quiet ones. Periods can get heavier or less predictable, which slowly drains iron. If you're thinking about pregnancy in the next year or two, your folate needs jump well before you ever see a positive test. And from your mid-to-late 30s, the slow approach to perimenopause (the years of hormonal change leading up to menopause) starts nudging mood, sleep, and inflammation.
None of that means you need to medicate it. It means a few specific nutrients become worth checking. The goal isn't to take more. It's to find the one or two things that are low for you and fix those.
So here's the short list, ranked by evidence, not by marketing budget: iron, folate, vitamin D3, omega-3, and magnesium. Next we'll get specific about what each one earns, and who should skip it.
Test before you buy (especially for iron)
The most common mistake we see isn't taking the wrong supplement. It's guessing. You feel tired, so you buy iron. Or you read a thread and buy all five. A simple blood panel tells you which ones are low, so you spend money only where it helps.
Iron is the clearest example, and it's where the standard test lets women down. When you get bloodwork, the number most doctors check is hemoglobin (the protein in red blood cells that carries oxygen). Hemoglobin can read perfectly normal while your iron stores are running on empty.
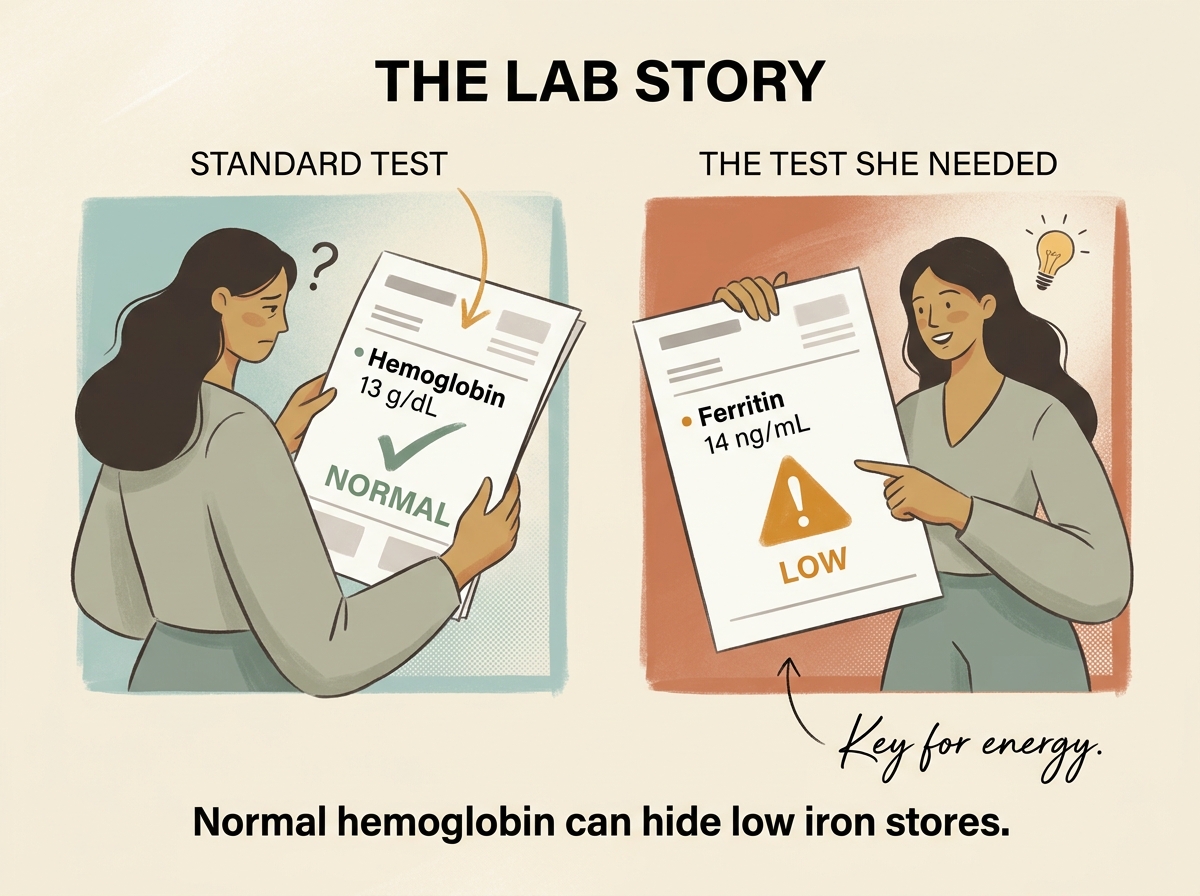
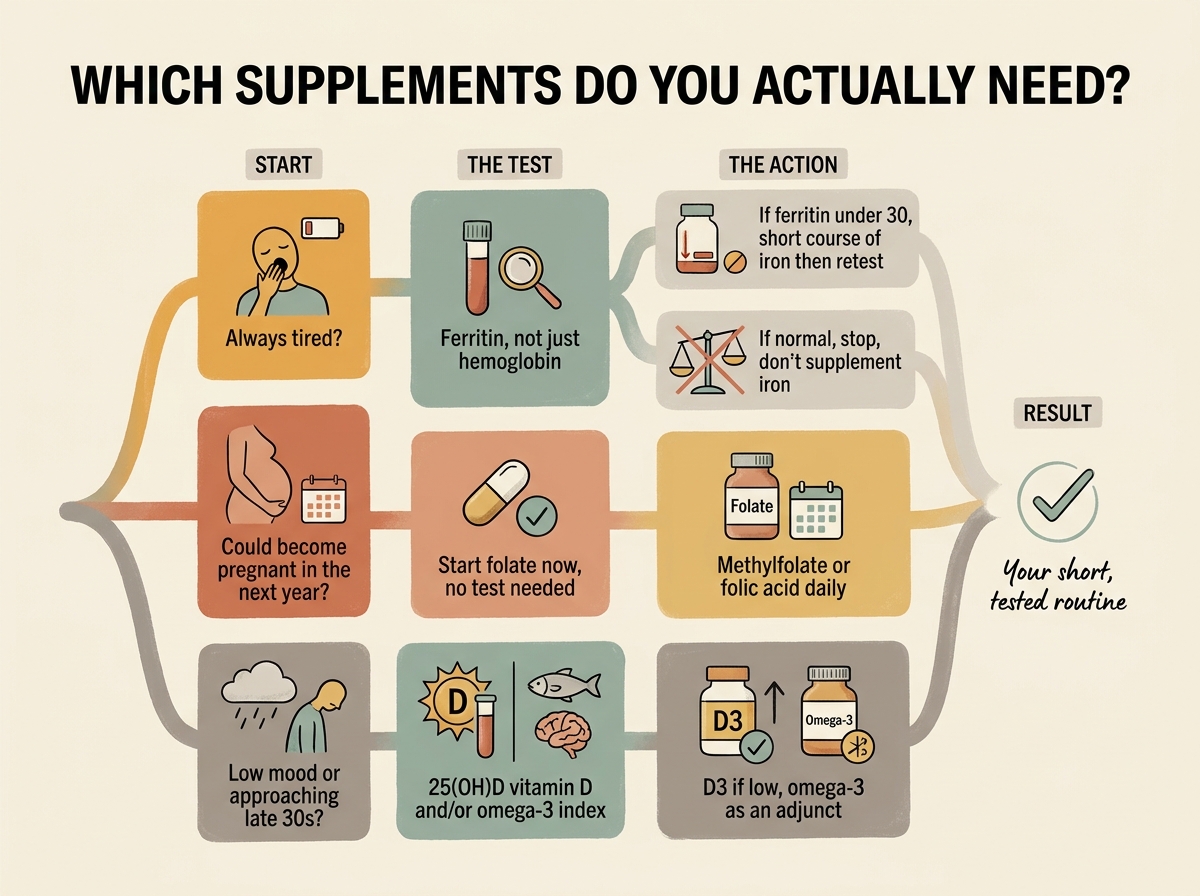
The test you want is ferritin, which measures how much iron you have stored away. You can have low stored iron with normal hemoglobin, and still feel wiped out, foggy, and cold. This is called non-anemic iron deficiency, and it's exactly the gap a hemoglobin-only test misses. Women who still menstruate are the group most likely to fall into it.
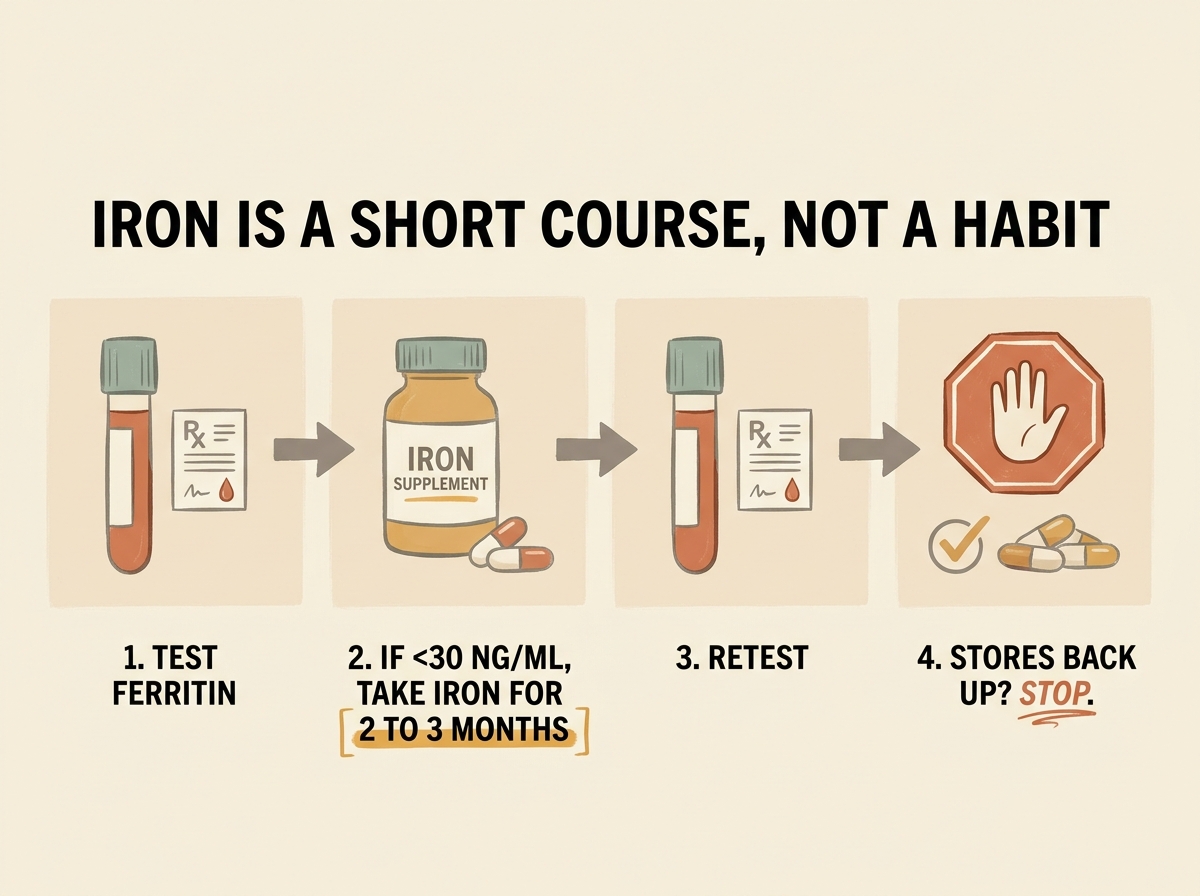
A reasonable floor is a ferritin above 30 ng/mL. Below that, low iron is the likely driver of the fatigue. Some practitioners aim higher for symptom relief. A target above 50 ng/mL is sometimes used when tiredness lingers despite a "normal" result. That higher number is a clinical judgment call, not a hard cutoff, so read it with your provider.
The same logic applies past iron. If low energy, low mood, or frequent colds are the problem, ask for a vitamin D test. It's reported as 25(OH)D, the storage form doctors measure. The point is the same throughout this article. A cheap test turns "I think I need this" into "I know I need this," and lets you skip the bottles you don't.
Already got a shelf of bottles and no idea which ones are pulling their weight? Show Your Supp' Buddy what you're taking. Scan a label or tell it the line-up, and it'll flag what matches the evidence for your goals and what's just taking up space.
The five supplements that earn a place in your 30s
Here are the five, in order of how strong the evidence is. For each one, the question isn't "is it good?" It's "do I need it?" Keep that in mind as you read.
Iron: only when your stores are low
Iron earns its spot only if your ferritin is low. If it's normal, taking iron does nothing good and can leave you constipated and queasy. This is the supplement women take blind most often, and need least often.
When stores are low, though, correcting them works. A double-blind trial in 164 women with low iron but no anemia found their fatigue eased and their ferritin climbed.1 Iron also corrects the deeper shortfall that often follows childbirth.3
Ferrous sulphate is the cheapest and most-studied form. If it wrecks your stomach, a gentler microencapsulated form is easier to tolerate without losing much absorption.7 Take it with a little vitamin C, and keep it away from coffee, tea, and calcium, which all blunt how much you take in. Harvard's Nutrition Source has a fuller list of foods that help and hinder iron absorption.
One rule beats any brand choice: correct, then retest. Iron isn't a forever supplement. Once your stores are back up, you stop, because too much iron carries its own risks.
Folate: start before you're pregnant
If there's any chance you could become pregnant in the next year, this is the one supplement here to start now, no test required. The stakes are why: started early, folate prevents the large majority of neural tube defects.2 No other item on this list carries that kind of payoff for so little effort or cost.
The catch is timing. The neural tube, the early structure that becomes the brain and spine, closes within the first month of pregnancy. That's often before a test turns positive. Topping up after you find out is too late, which is why the advice is to start a few months before you try.
For most women, 400 mcg (0.4 mg) a day of folic acid or methylfolate covers it. A common gene variant, present in an estimated 20 to 40 percent of people depending on ancestry, makes folic acid harder to process. If you carry this MTHFR gene variant, methylfolate, the pre-activated form, is the simpler choice. Women with a higher-risk history may need a larger dose their doctor sets.
One caution: very high folic acid can hide a vitamin B12 shortfall, so more isn't better. Stick to the standard dose unless your provider tells you otherwise. The CDC's folic acid guidance lands on the same standard dose.
Not sure which of these applies to you? Ask Your Supp' Buddy what's worth testing for your goals. Tell it whether you're planning a pregnancy, fighting fatigue, or just want to stop guessing. It'll point you to the few checks that matter before you spend a cent.
Vitamin D3: if a test says you're low
Vitamin D is worth taking if a test shows you're low. A lot of women are, especially in winter, with darker skin, or with little sun. Its strongest case is bone health, which matters more as you move through your 30s and beyond. The evidence there is well established.
For immunity, the picture is more modest. Across many trials, vitamin D slightly cut the risk of respiratory infections, with the clearest benefit in people who were deficient to start.8
Two things to get right. First, the form: choose D3 (cholecalciferol), not D2 (ergocalciferol). D3 is the kind your skin makes from sunlight, and it raises and holds your blood levels better.
Second, ignore the marketing that sells vitamin D as a fertility booster. A study of ovarian reserve, the egg supply marker doctors track, found vitamin D did not improve it.9
Some evidence suggests vitamin K2, the MK-7 form, may work alongside D3 for bone health, though direct trial evidence for the pairing is thin. Treat it as optional, not a must.
Omega-3: a modest mood and inflammation helper
Omega-3s, the healthy fats from oily fish, are a modest helper, not a headline act. They get more useful as you approach your late 30s and perimenopause. If you're already noticing those shifts, our guide to supplements for perimenopause by symptom picks up where this list ends.
The mood evidence is modest but consistent. A review found omega-3 had a small benefit for low mood during the menopausal transition.4 A more recent review agreed the effect is modest, and that it leans on the EPA-to-DHA ratio in your supplement.5
One women's-physiology specialist makes the case for why it matters more later in this window.
"Omega-3s are really essential for brain health, cellular health... especially as we get into [peri] and postmenopause. Estrogen used to help with anti-inflammatory properties."
— Dr. Stacy Sims, exercise physiologist
Not sure you even need it? There's a blood test, the omega-3 index, that tells you where you stand. If you want it to count, look for a supplement with more EPA than DHA. Our comparison of EPA versus DHA explains why the ratio matters for mood. Aim for 1000 to 2000 mg of EPA and DHA combined.
Magnesium: good for sleep, oversold for PMS
Magnesium is useful, just not for the reason it's sold most. Magnesium has a modest role in easing sleep, and it shows up most in people who were running low on it to begin with. It can also take the edge off everyday stress. Harvard's Nutrition Source covers magnesium's broader role in the body.
The glycinate form, magnesium bound to the amino acid glycine, is gentle on the stomach and a good default for sleep. If sleep is your main reason for taking it, our guide to which magnesium form has the best evidence goes deeper. A daily 200 to 400 mg is plenty. Go past the top of that range and you may get loose stools.
Community claim: "Magnesium fixed my PMS."
What the evidence says: For period-related mood symptoms, magnesium hasn't held up. A 2025 review found the evidence too thin to recommend it for the psychological symptoms of PMS.6 A separate study found no link between blood magnesium levels and PMS at all.10 If PMS mood is your target, vitamin B6, calcium, and zinc have better support.
One notable omission from this list: creatine. Dr. Stacy Sims and many in the community now flag it for women in their 30s. The case for muscle, and increasingly brain and mood, is strong. It sits just outside the five because it isn't tied to a deficiency you test for. We cover it on its own in our guide to creatine for women.
Getting these from food first
Before any of these go in a bottle, they go on a plate. Food is the cheaper, lower-risk way to top up most of them, and for two of the five it's all most women need. The table below shows one strong source for each, then we'll be honest about where food runs out.
| Nutrient | A strong food source | Serving | Roughly | Can food cover it? |
|---|---|---|---|---|
| Magnesium | Pumpkin seeds | 1 oz / 28 g (~85 seeds) | ~150 mg | Yes, realistically |
| Omega-3 (EPA+DHA) | Salmon (cooked) | 3 oz / 85 g | ~1,800 mg | Yes, with two fish meals a week |
| Folate | Edamame (cooked) | 1 cup / 155 g | ~480 mcg | Partly, but timing matters too |
| Iron | Lentils (cooked) | 1 cup / 198 g | ~6.6 mg | Maintains, won't rescue low stores |
| Vitamin D | Salmon (cooked) | 3 oz / 85 g | ~570 IU | Barely, sun and a pill do the work |
How much, how often: Magnesium is the easiest to eat your way to. An ounce (28 g) of pumpkin seeds gets you about half. Add a cup (172 g) of black beans and a cup (180 g) of cooked spinach, and most women hit the roughly 310 mg target. Still, many adults, by some estimates a majority in Western populations, fall short of the recommended magnesium intake from food alone. Omega-3 is simpler still: two meals of oily fish a week, like salmon, mackerel, or sardines, roughly covers a general intake. Iron and folate are where food helps but doesn't finish the job. A cup of lentils plus leafy greens chips away at the 18 mg iron target. But if your stores are already low, you can't eat your way out fast enough. Folate from edamame, lentils, and asparagus gets you close to 400 mcg on a good day. But not reliably every day, which matters most around conception.
Vitamin D is the outlier. Outside of oily fish, almost no food carries a meaningful amount, and you'd have to eat salmon daily to approach what your body needs. For vitamin D, sun and a supplement do the work that food can't.
So food covers magnesium and omega-3 for most women, chips away at iron and folate, and barely touches vitamin D. That's exactly the pattern the supplement should follow. It fills what your plate realistically can't, and nothing more.
Nutrient figures are approximate and drawn from USDA FoodData Central. Omega-3 amounts combine EPA and DHA, matching the dosage table.
How to take each one
If a test (or, for folate, your plans) says one of these is for you, here's the practical version. For each: the form that works, a starting dose, when to take it, and how long before you check whether it's doing anything. Doses below are starting points, not prescriptions. Your provider's number wins if it differs.
| Supplement | Form to pick | Starting dose | When | Give it |
|---|---|---|---|---|
| Folate | Methylfolate, or folic acid | 0.4 mg daily | Any time, daily | Start 3+ months before trying |
| Iron | Ferrous sulphate, or microencapsulated if it upsets your stomach | 60 to 80 mg elemental, only if ferritin is low | Morning, with vitamin C, away from coffee and calcium | 2 to 3 months, then retest |
| Vitamin D3 | Cholecalciferol (D3), not D2 | 1,000 to 2,000 IU daily | With a meal that has some fat | Recheck your level at 6 months |
| Omega-3 | Fish or algal oil, more EPA than DHA | 1,000 to 2,000 mg EPA+DHA | With a meal | 8 to 12 weeks for mood |
| Magnesium | Glycinate | 200 to 400 mg elemental | 30 to 60 minutes before bed | 4 to 8 weeks for sleep |
Two timing rules do most of the work. Keep iron away from calcium and from coffee or tea by a couple of hours, or you'll absorb far less of it. And if you take folic acid above the standard dose, pair it with vitamin B12, because high folic acid can paper over a B12 problem. Beyond that, take things with food unless a note above says otherwise, and you've covered the basics.
Who should take extra care
Most of these are low-risk at the doses above. A few situations change the math, and they're worth flagging before you start.
- Planning a pregnancy: folate is the priority, and earlier is better. Once you're pregnant, the usual guidance is to continue folate through the first trimester, with the dose set by your provider. Pair higher folic acid doses with B12 so a B12 shortfall doesn't go hidden.
- Taking iron without a test: don't. Your body has no easy way to dump extra iron, and too much is pro-oxidant and harmful. The upper limit for everyday supplementing is about 45 mg of elemental iron a day. Treatment doses for a confirmed shortfall run higher, but only under a provider's care. Supplementing without a confirmed low ferritin is the one mistake worth avoiding entirely.
- Kidney disease: magnesium clears through the kidneys, so if yours don't work well, magnesium can build up. Use it only under a doctor's guidance.
- On blood thinners or heading into surgery: high-dose omega-3, above roughly 3 g a day, can nudge bleeding risk. Mention your fish oil to whoever manages your medication.
- On thyroid medication, antibiotics, or acid reducers: iron interferes with several drugs. It blunts thyroid medication and some antibiotics, and acid reducers cut how much iron you absorb. Space iron a few hours from these and keep your prescriber in the loop.
If you're pregnant or breastfeeding, treat every supplement here as a conversation with your provider, not a self-serve decision. Safe doses shift in those windows.
The bottom line
Our read: the supplement aisle sells women in their 30s a problem they mostly don't have, which is not enough pills. It hides the one they do have, which is not knowing what's low. Two of these five, folate and iron, can change how a year of your life feels. The other three earn a place only when a test or your plans say so. The skill isn't collecting bottles. It's subtraction.
If you do one thing, make it a ferritin test and, if pregnancy is anywhere on your horizon, a folate habit. Everything else can wait until you have a reason, in writing, from your own blood.
Do I need to take iron if I'm not anemic?
Possibly, yes. Anemia is just the late stage of low iron. You can have empty iron stores while your hemoglobin still reads normal, and feel exhausted because of it. The fix is to ask for a serum ferritin test specifically, not only a standard iron panel. Serum just means it's measured in your blood, and ferritin is the iron your body keeps in storage. Supplement only if that number comes back low. See the test section above for the threshold.
Should I take D3 or D2?
D3. It's the same form your skin makes from sunlight, and it raises and holds your blood levels better than D2. D2 needs an extra conversion step that's less efficient. When you're choosing a bottle, the label word you want is cholecalciferol.
Does magnesium help PMS?
Not for the mood side, going by the evidence. The best available review found the case for magnesium and the psychological symptoms of PMS too thin to recommend. Vitamin B6, calcium, and zinc held up better. Magnesium does have a fair case for sleep and everyday stress, so it may help you feel better indirectly. It's just not the PMS fix it's marketed as.
Do I need folate if I'm not trying to get pregnant?
It's worth having covered if pregnancy is even possible down the line. The neural tube closes 21 to 28 days after conception, before most women know they're pregnant, so starting after a positive test is too late. That's why the advice reaches all women of reproductive age, not only those actively trying. If you carry the common gene variant that slows folic acid processing, the methylated form is the easier pick.
How do I know if I need omega-3 supplements?
There's a blood test for it, the omega-3 index, which measures EPA and DHA in your red blood cells. Most people on a standard Western diet land below 4 percent, and around 8 percent is considered the healthy zone. The shortcut: if you eat oily fish like salmon, sardines, or mackerel two to three times a week, you probably don't need a supplement. If you don't, a daily dose is a reasonable starting point.