Supplements for Perimenopause: What Works by Symptom
You're looking at supplements for perimenopause, and every bottle promises to "balance your hormones" or melt belly fat in one capsule. Maybe you've tried one and felt nothing. Maybe you're just tired of guessing which claim is honest. Either way, the honest answer is narrower, calmer, and cheaper than the aisle suggests, and this is the article that gives it to you.
Which supplements for perimenopause are worth it?
A short list of single supplements, each matched to one symptom, does more than any "hormone harmony" blend on the shelf. No pill fixes perimenopause the way hormone therapy can. But a handful have honest, if modest, support for specific problems. Black cohosh for hot flashes. Magnesium and ashwagandha for sleep. Ashwagandha for stress and low mood. Omega-3 for brain fog. And vitamin D for your bones.
Notice what that list does. It matches one supplement to one symptom. That's the whole game here. The smart move is simple. Pick the one or two things that target what's bothering you most. Take a studied dose long enough to judge it. Then skip the rest. Below, we sort it by symptom so you can jump straight to yours.
One honest expectation to set now: most of these effects are gentle. Ashwagandha for stress is the standout, with the most convincing trials behind it. The others are worth trying for the right symptom. But think "a bit better over a few weeks," not "a different person by Friday."
Why the "hormone harmony" blends overpromise
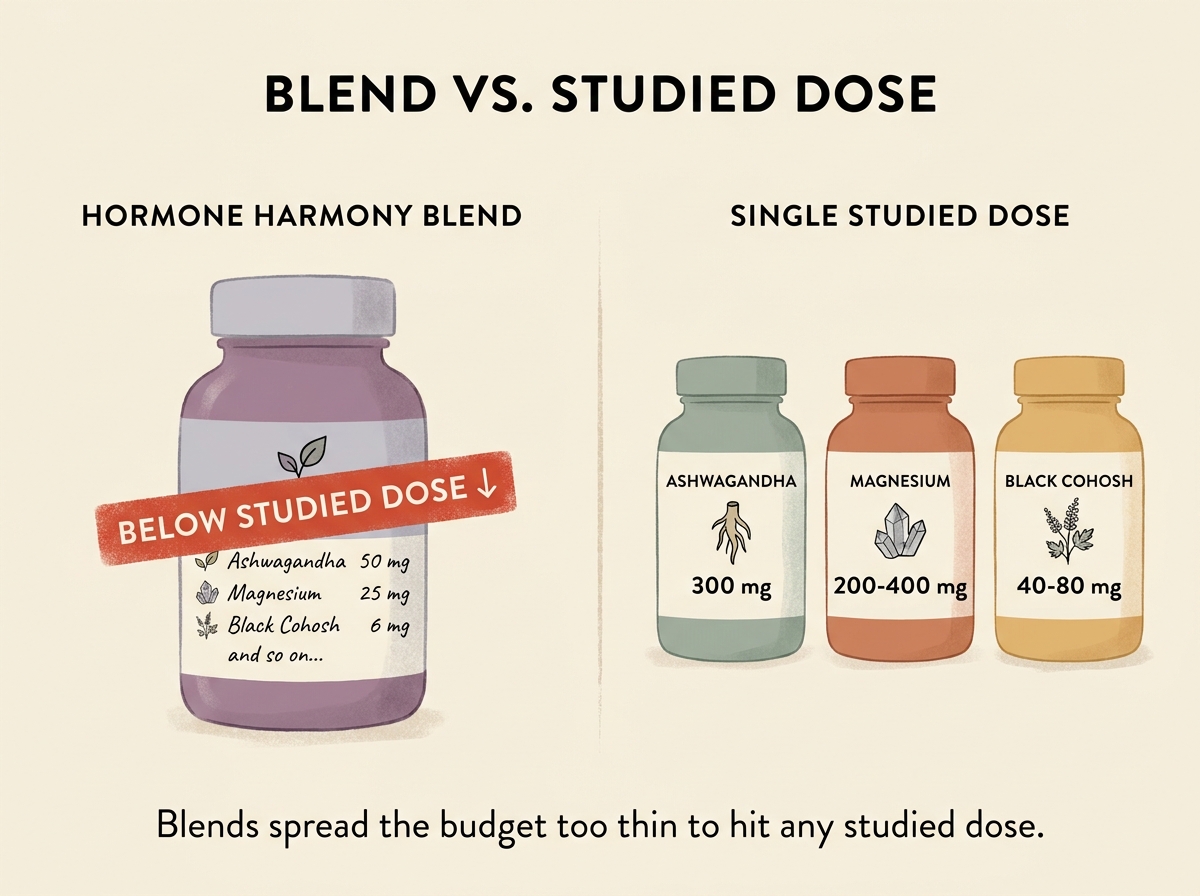
The blends are where most money gets wasted. A "complete menopause" capsule might list eight or ten ingredients, which looks thorough. The problem is the math. To fit them all in one pill, each ingredient gets a tiny amount, often a fraction of the dose any study tested.
Black cohosh is the clearest example. The trials that show a benefit use 40 to 80 mg of a standardized extract a day. A standardized extract just means each batch is made to a measured, consistent amount of the active plant compound. If a blend gives you 6 mg of it, you're nowhere near the studied dose, whatever the front of the box says.
A double board-certified OBGYN put it plainly in a talk on menopause supplements. The blends, she said, "don't have enough of any individual ingredient to be effective." They "mix so many things that they miss getting targeted levels." Targeted single supplements, at the doses studies used, do more for less money.
This is also where the marketing gets boldest. You'll see supplements sold for perimenopause "belly fat," "weight gain," and "hormone balancing." Be skeptical. No supplement in the current evidence has trial support for perimenopause fat loss. And "hormone balancing" is a marketing phrase, not a measured effect. If weight change is your main worry, that's its own topic, and a capsule isn't the lever.
For hot flashes and night sweats
For hot flashes and night sweats, black cohosh has the most trials behind it. A pooled analysis of 22 trials in women with menopausal symptoms found that standardized black cohosh improved overall symptoms and hot flashes specifically.3 A 2026 review from the International Menopause Society reached a similar read. It found moderate-confidence evidence that black cohosh helps vasomotor symptoms (the medical term for hot flashes and night sweats).1
Two honest caveats. First, black cohosh does not help mood or anxiety. The same large analysis found no benefit for either.3 If low mood is your main problem, this is the wrong pick, and many blends blur that line. Second, use a standardized extract, the kind quality reviews of these trials relied on.4 And if you've had estrogen-sensitive (ER+) breast cancer, talk to your oncologist first. The safety picture there is still unsettled.
Soy and red clover are the other hot-flash option you'll hear about. These contain phytoestrogens, plant compounds that act a little like the body's own estrogen but more weakly. The evidence here is more mixed for hot flashes than the marketing admits. A review of natural estrogen strategies reported that higher-dose dietary phytoestrogens lowered hot-flash intensity in the better-quality studies.8 Where soy isoflavones look steadier is overall menopausal symptoms and quality of life, not hot flashes alone.5
The myth: "Soy causes breast cancer, so skip the isoflavones."
What the evidence says: At normal food and supplement amounts, around 50 to 100 mg of isoflavones a day, the evidence does not show a higher breast-cancer risk.2 Soy compounds bind estrogen receptors far more weakly than the body's own estrogen. Soy intake is also linked to lower inflammation markers in women after menopause.13 The exception that matters: if you take tamoxifen, avoid isoflavones, and anyone with an ER+ breast-cancer history should clear it with their oncologist first.
For sleep that keeps breaking
For broken perimenopausal sleep, magnesium is the quiet first step. It's cheap, well tolerated, and most women run low on it. Estrogen loss and ongoing stress both pull magnesium out of the body, so the gap tends to widen in this phase. Magnesium also supports GABA (the brain's main calming signal), which is part of why it helps wind-down. A menopause-focused review lists it among the supplements that show promise for sleep and mood.2 Our guide to magnesium for sleep goes deeper on form and timing if that's your main reason for trying it.
For sleep, the glycinate form is the usual pick because it's gentle on the stomach and absorbs well. A common approach is 200 to 400 mg of elemental magnesium, taken 30 to 60 minutes before bed. Start at 200 mg and only go up if you tolerate it. The form guidance here comes from clinician experience, not head-to-head perimenopause trials, so treat it as a sensible starting point.
Ashwagandha is the stronger of the two for sleep, mostly because it works on what's keeping you up: a wired, can't-switch-off feeling. It's an adaptogen, a plant that helps blunt the body's stress response, and it lowers cortisol, the main stress hormone.6 A menopause specialist describes taking it at night, sometimes alongside magnesium glycinate, to help the body shift into rest mode. Give either one a few weeks, not a few nights. If one alone isn't enough, our deep sleep stack protocol covers what layers well.
For mood swings, anxiety, and low mood
For mood and anxiety, ashwagandha is the best-supported supplement in this whole list. The reason fits perimenopause well. As estrogen swings, the body's stress system gets more reactive. Doctors call it the HPA axis (the brain's main stress-hormone system, a loop running from your brain down to the adrenal glands). And when cortisol runs high, everything else feels worse. Ashwagandha turns down that stress response.
In an 8-week trial of 141 adults, a standardized root extract lowered cortisol and improved stress and anxiety scores against a dummy pill.6 A second 2026 trial found cortisol dropped by roughly 29% on a standardized extract.7 Another trial reported less fatigue in stressed adults.10 These studies weren't run in perimenopausal women specifically, so the fit is reasoned, not proven. But the stress mechanism applies directly. The usual dose is 300 to 600 mg of a standardized root extract daily, often split as 300 mg twice a day.
Magnesium is the gentler add-on for mood. A review of treatments for milder low mood found magnesium helped ease mild depressive symptoms.14 It won't replace treatment, but it's a low-risk piece that pairs naturally with the sleep benefit above. One thing to skip for mood: black cohosh. Despite how it's marketed, the trials show it does nothing for anxiety or depression.3 If anxiety is the bigger problem, our roundup of supplements for anxiety covers more options.
For brain fog
For brain fog, omega-3 fish oil is the most studied of these options, though the evidence is still being pinned down. Your brain is built partly from DHA, one of the two main omega-3 fats, and estrogen normally helps your body make it. As estrogen drops, that supply may dip too. A review of omega-3 and the menopausal brain describes accumulating evidence for benefits to thinking and mood. It's honest that results vary by dose and the EPA-to-DHA mix.12 A common target is 1 to 2 g of combined EPA and DHA a day, leaning EPA-heavy when mood is part of the picture. For the detail on EPA versus DHA, see our comparison of EPA and DHA.
Some clinicians also reach for magnesium in its threonate form for brain fog, since it's designed to reach the brain better than other forms. The two forms aren't interchangeable, though. Threonate is dosed lower and aimed at brain delivery, not the higher dose you'd use of glycinate for sleep. That's a mechanism-and-experience call, not a perimenopause-tested one, so set expectations accordingly. If you only want to add one thing for fog, start with omega-3.
For your bones, the change you can't feel
Bone loss is the perimenopause symptom you won't notice until it matters, which is exactly why it's worth acting on early. Estrogen protects bone, so as it falls, bone breaks down faster. Vitamin D is the foundation here. The International Menopause Society's 2026 review found high-confidence evidence that vitamin D is safe. It found moderate-confidence evidence that vitamin D lowers fracture risk, especially paired with calcium.1
A board-certified menopause specialist calls vitamin D "the number one supplement I recommend" for this transition. It's hard to get enough from food or sun alone. A typical dose is 1,000 to 2,000 IU of D3 a day, taken with a meal that has some fat. An integrative perimenopause review groups vitamin D with magnesium, calcium, and vitamin K2 as the bone-supporting set.2 Many clinicians add K2 (MK-7, about 100 to 200 mcg) to steer calcium into bone.
Not sure which of these maps to your symptoms, or whether it's safe with the medication you already take? Tell Your Supp' Buddy your top symptom and everything you're on. It checks the evidence, flags interactions across your list, and hands back a short shortlist built for you, not a textbook.
Getting these from food first
Before you buy anything, it's worth knowing which of these you can get from your plate. For some, food does most of the work. For others, a supplement is the only practical route. Here's the honest split.
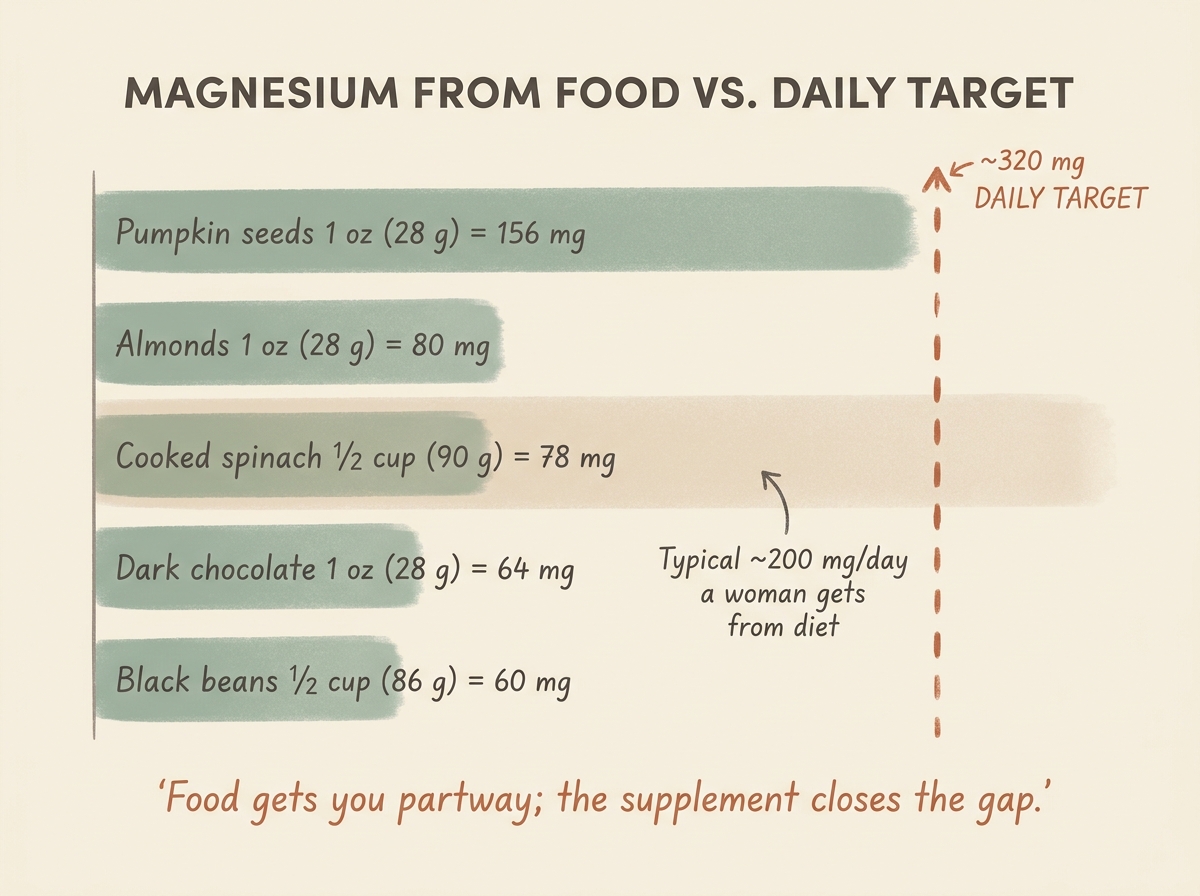
Magnesium is the best food story of the group. Women 31 and older need about 320 mg a day, but most get only around 200 mg from food, a gap perimenopause widens. The richest sources are easy to add. Pumpkin seeds lead with about 156 mg per ounce (28 g). Almonds give about 80 mg per ounce (28 g), and a half cup (90 g) of cooked spinach about 78 mg. Dark chocolate and black beans add roughly 60 mg each. A daily ounce (28 g) of pumpkin seeds plus a spinach side closes about half the gap. A small daily supplement covers the rest, which is why food plus a modest top-up beats either alone.
Omega-3 has a decent food path. Two to three servings of oily fish a week, like salmon, mackerel, or sardines, gets most women into the studied range. Lead with the fish; the capsule is for those who dislike it or want a steadier dose. If you eat a lot of fish, mind mercury and buy quality.
Soy isoflavones sit in the middle. Whole and fermented soy foods, like edamame, tofu, miso, and tempeh, give roughly 25 to 50 mg each. One or two servings a day approaches the studied range. Fermented soy also helps your gut make equol, a stronger compound only some people produce. Western diets are usually low here.
Vitamin D is the one food can't fix. Oily fish, fortified dairy, and egg yolks don't add up to enough, and sun is unreliable. For most perimenopausal women, the supplement is the realistic route, not a backup. Black cohosh and ashwagandha aren't foods at all. They're plant extracts, so a capsule is the only way to get a studied dose.
Doses, forms, and timing at a glance
Here's the practical version of everything above. The table makes the studied dose easy to copy. It also shows how long to give each one before you judge it. The single most common mistake is quitting at day four. These work over weeks.
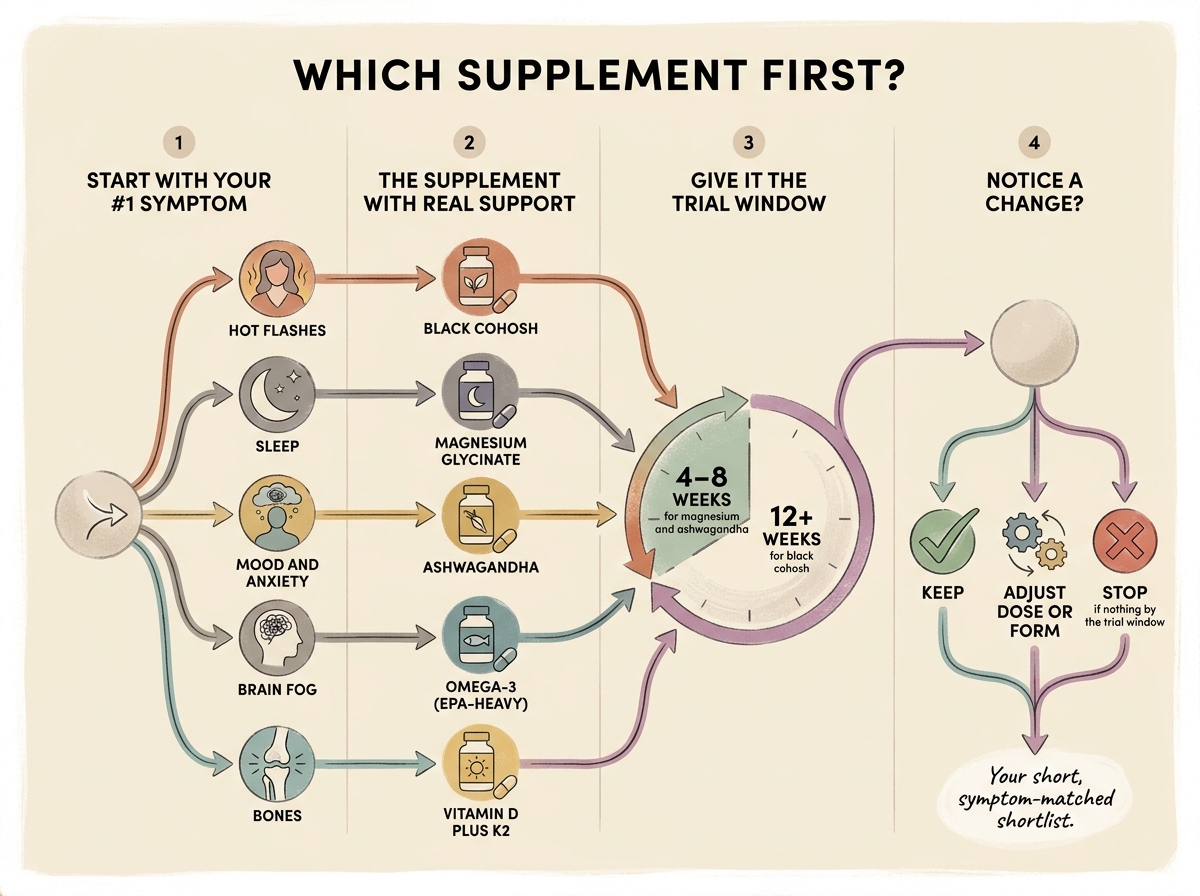
Read the table as a starting point, then use the flow above to decide what to keep. Pick your top symptom, take the matched supplement at the studied dose, and give it the trial window. If nothing has shifted by the end of that window, stop, or switch form, rather than stacking more on top.
| Supplement | Form | Daily dose | When | Give it | Notes |
|---|---|---|---|---|---|
| Black cohosh | Standardized extract | 40–80 mg | Morning or split | 12+ weeks | Standardized only; for hot flashes, not mood |
| Magnesium | Glycinate (sleep, mood) | 200–400 mg elemental | 30–60 min before bed | 4–8 weeks | Daily cap from supplements is 350 mg |
| Magnesium | Threonate (brain fog) | ~144 mg elemental | Morning and evening | 4–12 weeks | Form choice is clinician experience, not a trial |
| Vitamin D3 | Softgel | 1,000–2,000 IU | With a fatty meal | Ongoing | Pair with K2 (MK-7 100–200 mcg) |
| Ashwagandha | Standardized root (KSM-66 / Sensoril) | 300–600 mg | 300 mg twice daily, or 600 mg with food | 8–12 weeks | Root-only; avoid blends |
| Omega-3 | Fish or algae EPA+DHA | 1–2 g EPA+DHA | With meals | Ongoing | EPA-heavy for mood |
| Soy isoflavones | Extract or fermented soy | 50–100 mg | With a meal | 12+ weeks | Fermented soy aids equol conversion |
Safety and what to check on the label
Perimenopausal women are often on at least one prescription, so this is the section to read closely before you add anything. None of these supplements is a substitute for treatment, and a few carry interactions worth naming.
- On a thyroid medication like levothyroxine? Ashwagandha can raise thyroid hormone levels and push your dose off. Ask your prescriber about checking your levels.
- On a blood thinner like warfarin? Keep omega-3 at or below 2 g a day. Higher doses can add to the bleeding effect.
- Taking tamoxifen means skipping isoflavones entirely. As plant estrogens, they may work against the drug.
- Black cohosh and your liver. Liver injury is rare, but avoid combining it with other hard-on-the-liver drugs, and stop it two weeks before any surgery.
- Magnesium can block the absorption of some antibiotics, so take it at least two hours apart from them.
Two label rules cover most of the risk. Buy standardized ashwagandha root extract (KSM-66 or Sensoril) and standardized black cohosh. Skip the no-name multi-ingredient blends, since the rare safety reports cluster around those. And if you have a history of ER+ breast cancer, treat black cohosh and isoflavones as a conversation for your oncologist, not a self-serve choice. On the basics, standardized ashwagandha has been well tolerated across many trials, with stress, organ, and hormone markers staying in normal range.9
One to watch, not buy yet: probiotics. An early analysis hints at benefits for menopausal symptoms. But the studies so far are shaky, so treat it as "keep an eye on it," not a recommendation.11
The bottom line
Our read on the evidence: perimenopause supplements are repair work, not magic. They help most when they correct a shortfall, like low magnesium or low vitamin D, and they help one symptom at a time. The aisle sells the opposite story, a single capsule that balances everything, and that story is where the money goes to die.
If you want to test this the honest way, pick your loudest symptom and one matched supplement. Take the studied dose, give it the weeks the trials gave it, and judge it then. Ashwagandha for a wired, stressed mind is the one most likely to surprise you. The rest earn their place quietly, or not at all. Either way, you'll know, and you'll have spent less finding out.
Common questions
What helps most with hot flashes in perimenopause?
Black cohosh has the most trials behind it for hot flashes and night sweats, at the standardized dose in the table above.3 Higher-dose dietary phytoestrogens from soy may also lower hot-flash intensity.8 For severe symptoms, hormone therapy still outperforms any supplement, so it's worth a doctor conversation.
Is magnesium good for perimenopause?
Magnesium is one of the most broadly useful picks, mainly for sleep and mood, and most women are low in it to begin with. The glycinate form suits sleep; some clinicians use the threonate form for brain fog. It's gentle, cheap, and pairs well with vitamin D for bones. See the dose section above for the starting amount.
Is ashwagandha good for perimenopause?
It's the best-supported supplement here for stress, anxiety, and the sleep problems that stress drives. Two 2026 trials showed lower cortisol and better stress and anxiety scores.67 It hasn't been tested in perimenopausal women specifically, but the stress mechanism applies directly. Use a standardized root extract, and check with your prescriber if you take thyroid medication.
Should I take a menopause blend or individual supplements?
Individual supplements at studied doses beat the "hormone harmony" blends. Blends spread the budget across so many ingredients that each one lands below the dose any study tested. Match a single supplement to your main symptom instead, and skip the all-in-one capsule.
Do any supplements help perimenopause weight gain or belly fat?
Honestly, no. No supplement in the current evidence has trial support for perimenopause fat loss. And "hormone balancing" for weight is a marketing claim, not a measured effect. Weight change in this phase is driven by sleep, muscle, and shifting hormones, which a capsule won't fix.