
EPA vs DHA: Which Omega-3 Actually Matters for Your Goal?
Pick up your fish oil bottle and flip it over. The front says 2,000 mg fish oil. The small print on the back says 300 mg EPA, 200 mg DHA. That's 500 mg of actual omega-3. The cardiovascular trials that changed prescribing guidelines used 1,800 to 4,000 mg of EPA alone23. Your bottle isn't even close. This article tells you which omega-3 your goal needs, at what dose, and in what form.
Your fish oil is two different molecules
EPA and DHA aren't interchangeable. They do different things in your body.
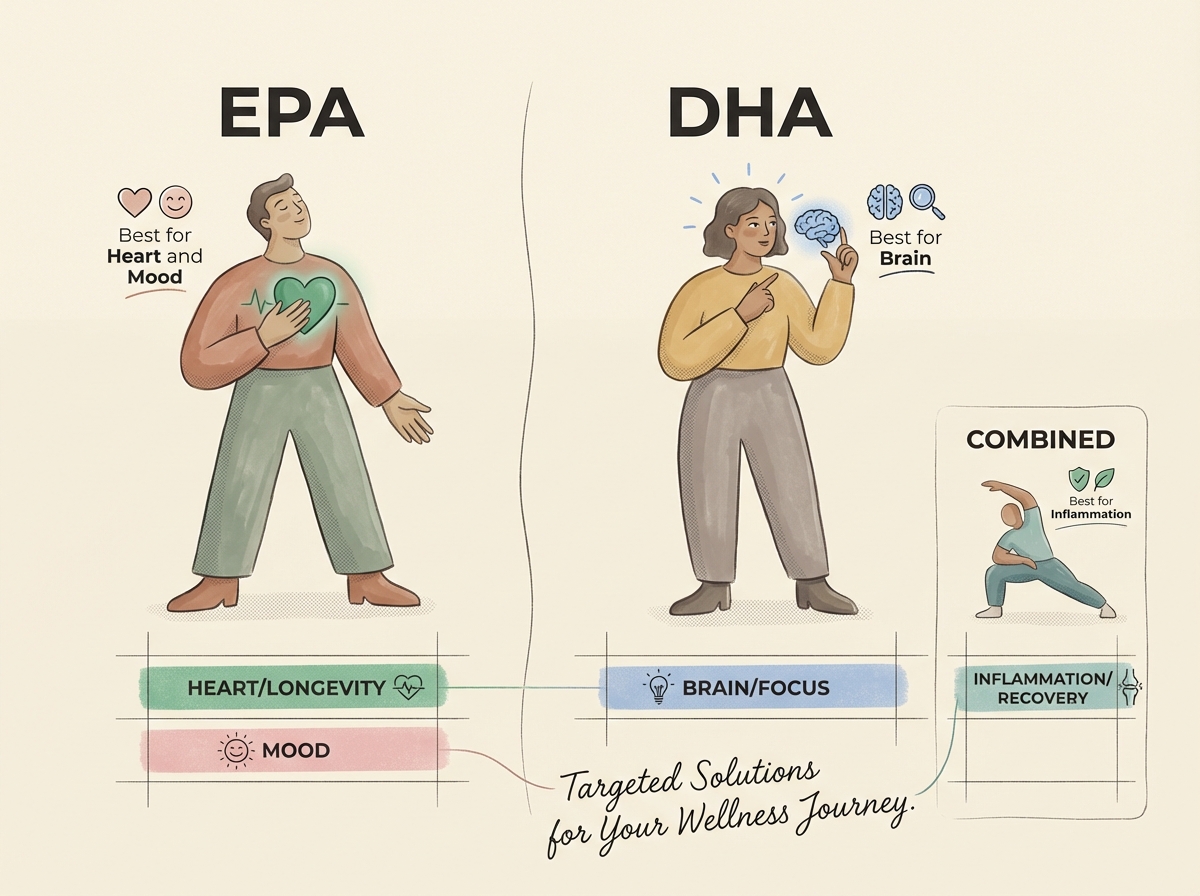
EPA is the anti-inflammatory one. It competes with omega-6 fats for the same enzymes and pushes your body toward less inflammatory signals11. That's why it dominates heart and mood research.
DHA is the structural one. It makes up the vast majority of omega-3 fatty acids in brain tissue, woven into the membranes of every neuron. Your brain depends on it for signaling and long-term maintenance.
What people say online: "I just grab whatever fish oil is on sale."
What the evidence says: The cheapest bottle might have the right molecule for your goal, or it might not. Cardiovascular trials used pure EPA. Brain studies used DHA. A general blend will do something for inflammation, but if you care about your heart, one trial used a blend of both and it failed where pure EPA succeeded4.
Four goals, four answers
Heart health: EPA, not both
A landmark trial gave 8,179 statin-treated patients pure EPA at 4 g/day. Major cardiovascular events dropped by 25%2. An earlier trial of 18,645 patients found that EPA at 1.8 g/day cut coronary events by 19%3.
A separate trial tested a mix of EPA and DHA together instead of pure EPA. No cardiovascular benefit4. Same class of fat, different result. A 2024 review confirmed that EPA and DHA have distinct effects on cardiovascular risk factors7. The key difference: only DHA raises LDL cholesterol1. One possible explanation is that the LDL-raising effect diluted EPA's benefit when they were combined.
For heart health, the molecule is EPA. Not a balanced blend.
Mood and depression: EPA leads here too
Meta-analyses of omega-3 trials for depression reach the same conclusion: EPA-dominant formulas outperform DHA-dominant products for depressive symptoms5. The pattern holds across clinical depression, bipolar disorder, and peripartum populations.
The effective ratio in most mood studies is at least 60% EPA5. A standard 2:1 EPA:DHA supplement meets that. High-DHA products don't show the same antidepressant effect. If mood is your goal, check the label for the EPA number specifically.
You just figured out which omega-3 fits your goal. Now find out if your bottle delivers it. Scan your bottle with Your Supp' Buddy and it'll check the EPA and DHA split against your goal and show you whether the dose matches what the evidence studied.
DHA for brain health: small but consistent
If you're under 50 and eat fish a couple of times a week, DHA supplements probably won't move the needle for you. The benefit is clearest in older adults and people who rarely eat fish.
A 2024 meta-analysis of 37 trials found DHA supplementation improved cognitive markers in older adults6. A dose-response review found that higher DHA levels in the body tracked with lower risk of cognitive decline13. The effect is strongest in people over 60 or anyone with low fish intake.
DHA supplementation is about protecting what you have, not a performance boost.
Inflammation and recovery: both, together
For joint pain, exercise soreness, or general anti-inflammatory goals, EPA and DHA work as a team. EPA generates one family of inflammation-resolving molecules. DHA generates a different family11. Together they cover both pathways.
A 2026 meta-analysis of 41 trials found combined EPA+DHA at 2 g/day or more for at least six weeks reduced key inflammatory markers8. A separate review in rheumatoid arthritis confirmed reductions in inflammation and disease activity9.
Not sure how your omega-3 fits with everything else you take? Show Your Supp' Buddy your full stack — scan each bottle and it'll check doses, flag interactions, and tell you if anything overlaps.
The dose your bottle probably isn't giving you
Finding the best omega-3 supplement for your goal means ignoring the big number on the front and going straight to the EPA and DHA breakdown on the back.
| Goal | What to take | Daily dose | How long | Evidence |
|---|---|---|---|---|
| Heart health | EPA-only or EPA-dominant fish oil | 1.8 to 4 g EPA | Ongoing | A |
| Mood / depression | EPA-dominant (EPA:DHA 2:1 or higher) | 1 to 2 g EPA | 8 to 16 weeks minimum | A- |
| Brain / cognition | Fish oil or algal oil (DHA-rich) | 500 mg to 1 g DHA | 6 to 24 months | B |
| Inflammation / recovery | Combined EPA+DHA, TG form preferred | 2 to 3 g combined | 6 weeks minimum | A- |
| General health | Any EPA+DHA supplement | 250 to 500 mg combined | Ongoing |
Form matters. At doses under 2 g/day, the natural triglyceride (TG) form works better than synthetic ethyl ester for lowering CRP10. Look for "triglyceride form" or "rTG" on the label. If it only says "fish oil concentrate" or "ethyl ester," it's the cheaper form.
Why most bottles use a 2:1 EPA:DHA ratio. Early omega-3 research focused on EPA, and the fish species used for most supplements naturally yield more EPA than DHA. That ratio works for inflammation and mood. It doesn't match the evidence for cardiovascular goals (pure EPA) or brain goals (DHA-dominant).
Vegan note. Algal oil covers DHA as well as fish oil. But most algal products contain little or no EPA. If you're plant-based and want EPA for heart or mood goals, you'll need a separate algae-sourced EPA supplement. Your body barely converts ALA from flaxseed and walnuts into EPA or DHA. Plant sources alone won't get you to therapeutic levels.
Safety and interactions
Omega-3 supplements have a strong safety record at standard doses. Two things to mention to your doctor:
Heart rhythm. In statin-treated patients with existing cardiovascular disease, 4 g/day of pure EPA added about 1 percentage point to the rate of atrial fibrillation hospitalizations (3.1% vs 2.1% on placebo)3. If you have a history of heart rhythm issues, talk to your cardiologist before starting high-dose omega-3.
Blood thinners. If you're on warfarin, aspirin, or other anticoagulants, let your prescriber know you're supplementing with omega-3. At high doses (4 g/day or more) it may increase bleeding time. At standard supplement doses (under 3 g/day), researchers checked whether combining omega-3 with statins caused problems. At standard doses, it didn't12.
Take omega-3 with food. Fat in the meal improves absorption.
The bottom line
The word "omega-3" has been doing a lot of marketing work for a long time. The trials that built the reputation weren't run on "omega-3." They were run on specific doses of EPA for cardiovascular risk, specific doses of DHA for brain maintenance, specific ratios for specific outcomes. The generic mixed blend that sits on every shelf matches almost none of those trials exactly.
A supplement industry built around a category will always produce products that average out the trials rather than replicate any of them. If you're actually chasing a result, don't buy the category. Buy the molecule the study used.